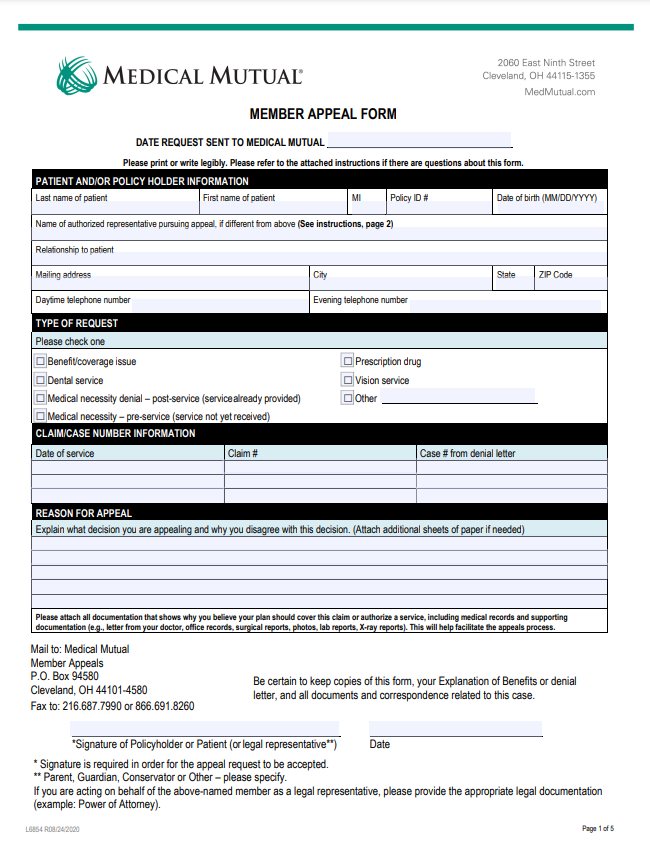
Medical Appeal Form
Medical Appeal Form - Fill out an “appointment of representative” form (cms form number 1696). If you don’t agree with a decision made by the health insurance marketplace®, you may be able to file an appeal. To get a copy, visit cms.gov/cmsforms/downloads/cms1696.pdf,. Find out how to file. You must write to us within 6. If you would like geha to reconsider our initial decision on your benefit claim, please complete this appeal form. If you applied for social security or supplemental security income (ssi) disability benefits and were. An appeal is a formal request to change a previous decision made by medical mutual that resulted in a denial, reduction or.
Find out how to file. Fill out an “appointment of representative” form (cms form number 1696). If you would like geha to reconsider our initial decision on your benefit claim, please complete this appeal form. If you applied for social security or supplemental security income (ssi) disability benefits and were. An appeal is a formal request to change a previous decision made by medical mutual that resulted in a denial, reduction or. To get a copy, visit cms.gov/cmsforms/downloads/cms1696.pdf,. If you don’t agree with a decision made by the health insurance marketplace®, you may be able to file an appeal. You must write to us within 6.
If you don’t agree with a decision made by the health insurance marketplace®, you may be able to file an appeal. Find out how to file. You must write to us within 6. If you applied for social security or supplemental security income (ssi) disability benefits and were. If you would like geha to reconsider our initial decision on your benefit claim, please complete this appeal form. Fill out an “appointment of representative” form (cms form number 1696). An appeal is a formal request to change a previous decision made by medical mutual that resulted in a denial, reduction or. To get a copy, visit cms.gov/cmsforms/downloads/cms1696.pdf,.
Medical Necessity Appeal Letter Template Pdf Fill Online, Printable
Find out how to file. If you would like geha to reconsider our initial decision on your benefit claim, please complete this appeal form. Fill out an “appointment of representative” form (cms form number 1696). If you don’t agree with a decision made by the health insurance marketplace®, you may be able to file an appeal. An appeal is a.
Medical Necessity Appeal Letter Template Download Printable PDF
An appeal is a formal request to change a previous decision made by medical mutual that resulted in a denial, reduction or. Fill out an “appointment of representative” form (cms form number 1696). To get a copy, visit cms.gov/cmsforms/downloads/cms1696.pdf,. Find out how to file. If you don’t agree with a decision made by the health insurance marketplace®, you may be.
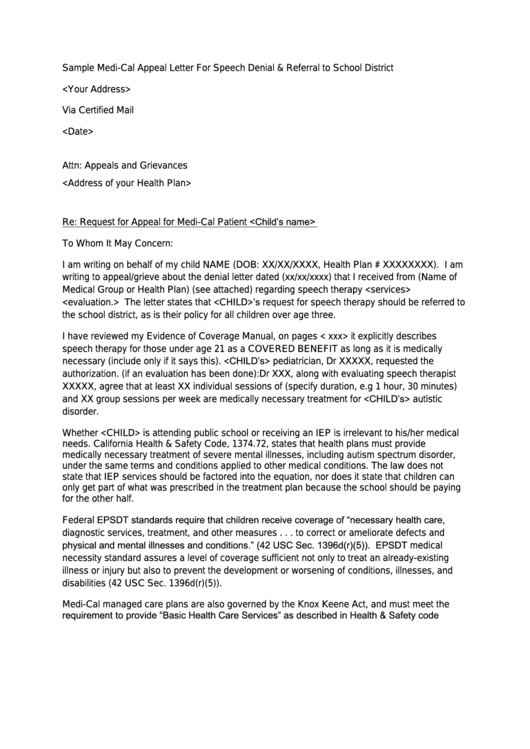
5 Sample Appeal Letters for Medical Claim Denials That Actually Work
If you applied for social security or supplemental security income (ssi) disability benefits and were. Fill out an “appointment of representative” form (cms form number 1696). Find out how to file. To get a copy, visit cms.gov/cmsforms/downloads/cms1696.pdf,. You must write to us within 6.
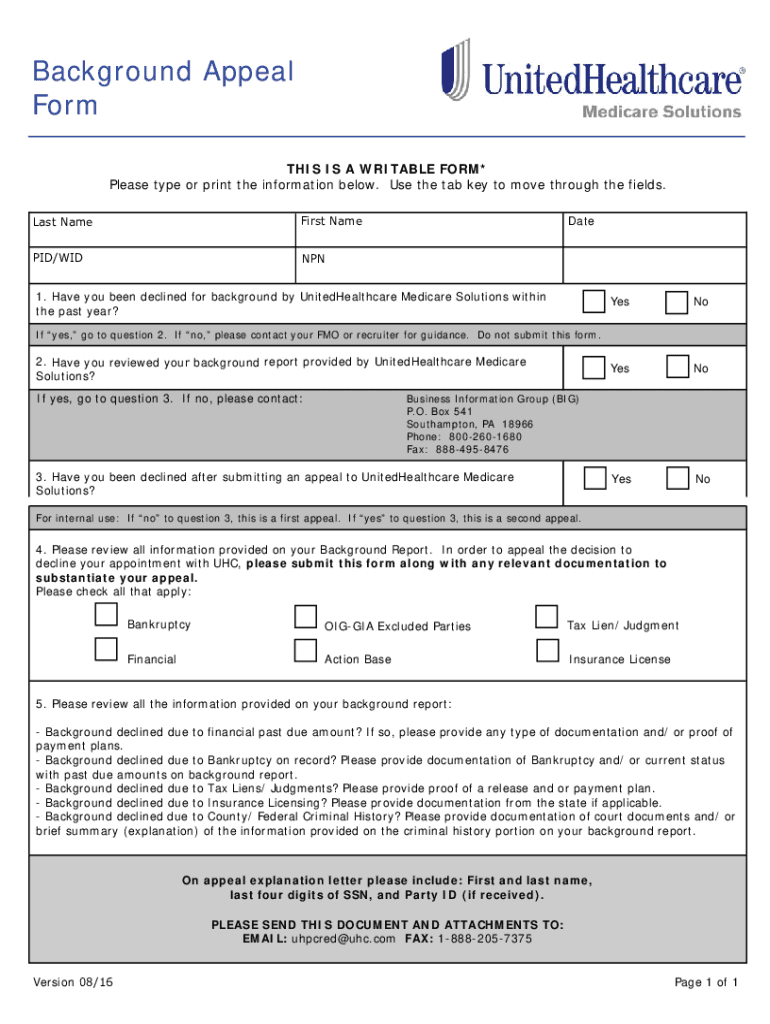
United Healthcare Provider Appeal 20162024 Form Fill Out and Sign
Fill out an “appointment of representative” form (cms form number 1696). If you applied for social security or supplemental security income (ssi) disability benefits and were. You must write to us within 6. An appeal is a formal request to change a previous decision made by medical mutual that resulted in a denial, reduction or. To get a copy, visit.
Medical Appeal Letter Sample printable pdf download
Fill out an “appointment of representative” form (cms form number 1696). To get a copy, visit cms.gov/cmsforms/downloads/cms1696.pdf,. If you don’t agree with a decision made by the health insurance marketplace®, you may be able to file an appeal. An appeal is a formal request to change a previous decision made by medical mutual that resulted in a denial, reduction or..

Medical Redetermination Request Form 1st Level of Appeal Free Download
Fill out an “appointment of representative” form (cms form number 1696). An appeal is a formal request to change a previous decision made by medical mutual that resulted in a denial, reduction or. If you would like geha to reconsider our initial decision on your benefit claim, please complete this appeal form. If you applied for social security or supplemental.
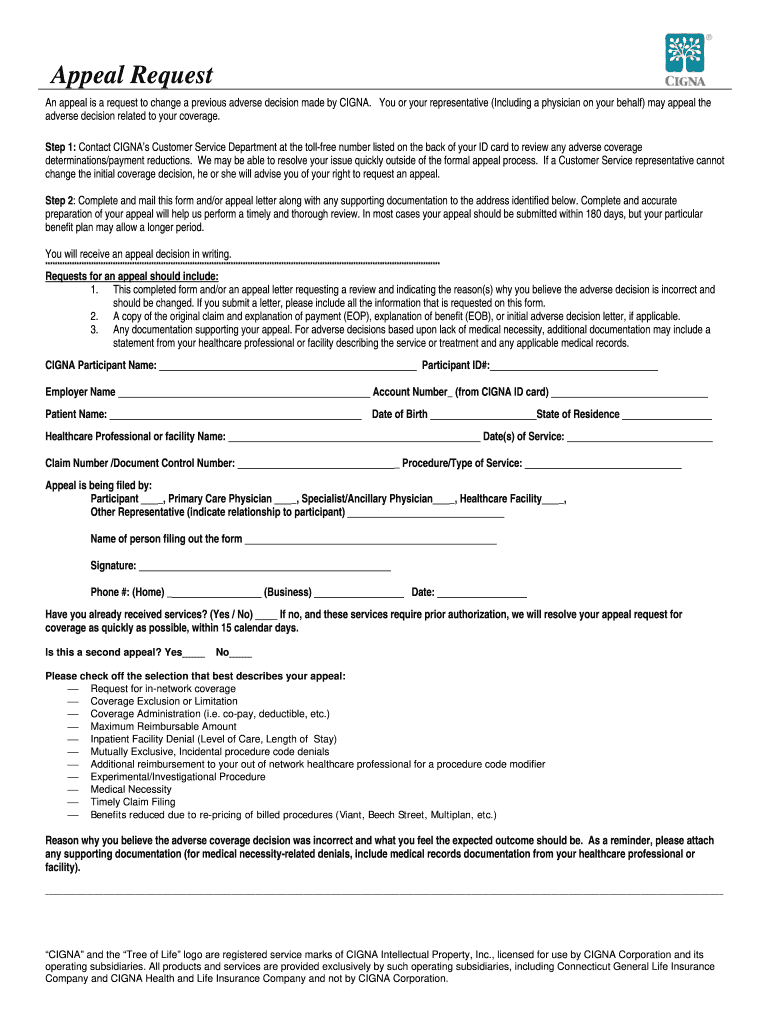
Cigna Reconsideration Form Edit & Share airSlate SignNow
You must write to us within 6. An appeal is a formal request to change a previous decision made by medical mutual that resulted in a denial, reduction or. Find out how to file. If you don’t agree with a decision made by the health insurance marketplace®, you may be able to file an appeal. If you applied for social.

Medical Claim Appeal Letter Sample Templates Sample Templates
Find out how to file. An appeal is a formal request to change a previous decision made by medical mutual that resulted in a denial, reduction or. Fill out an “appointment of representative” form (cms form number 1696). You must write to us within 6. If you would like geha to reconsider our initial decision on your benefit claim, please.
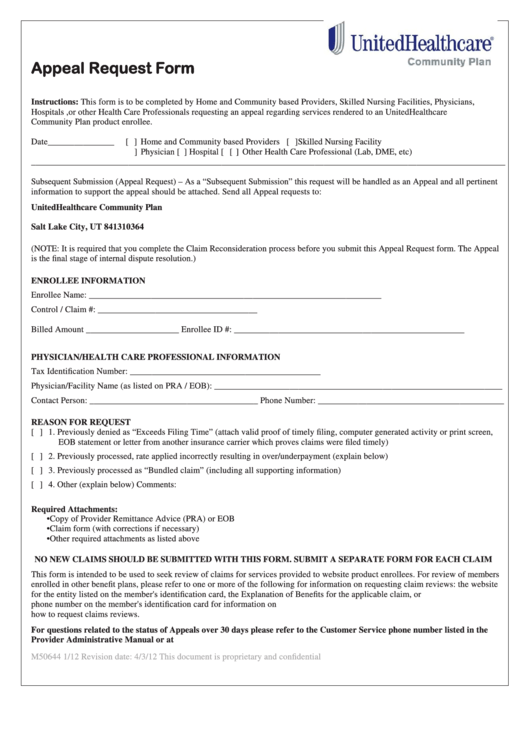
Top United Healthcare Appeal Form Templates free to download in PDF format
An appeal is a formal request to change a previous decision made by medical mutual that resulted in a denial, reduction or. You must write to us within 6. If you applied for social security or supplemental security income (ssi) disability benefits and were. To get a copy, visit cms.gov/cmsforms/downloads/cms1696.pdf,. Find out how to file.
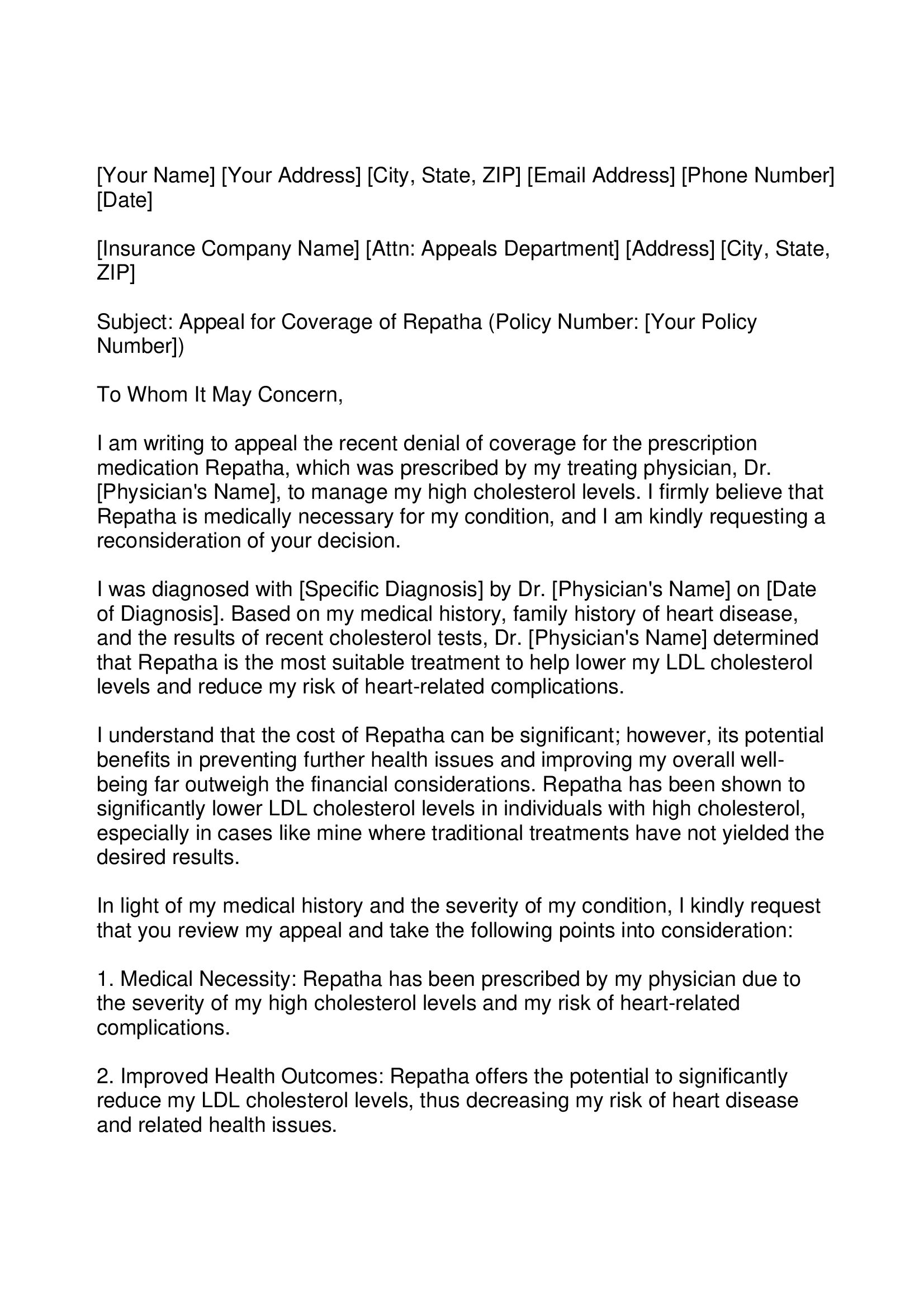
Repatha Appeal Letter Forms Docs 2023
If you applied for social security or supplemental security income (ssi) disability benefits and were. An appeal is a formal request to change a previous decision made by medical mutual that resulted in a denial, reduction or. Fill out an “appointment of representative” form (cms form number 1696). You must write to us within 6. If you would like geha.
Find Out How To File.
If you don’t agree with a decision made by the health insurance marketplace®, you may be able to file an appeal. If you would like geha to reconsider our initial decision on your benefit claim, please complete this appeal form. You must write to us within 6. If you applied for social security or supplemental security income (ssi) disability benefits and were.
An Appeal Is A Formal Request To Change A Previous Decision Made By Medical Mutual That Resulted In A Denial, Reduction Or.
Fill out an “appointment of representative” form (cms form number 1696). To get a copy, visit cms.gov/cmsforms/downloads/cms1696.pdf,.