Express Scripts Form
Express Scripts Form - If your address is different than what is on the form,. New prescription your patient would like to receive their prescription medication by mail. Log in or register to access the forms. Based upon each patient’s prescription plan, additional questions may be required to complete the prior authorization process. Find and print forms for mail order, claims, and medical questionnaire for tricare pharmacy benefits. 34202 please complete all information. Express scripts is administering this program on behalf of your medicare part d plan. You can ask your doctor to submit this form to us, or you can print and complete the form, then mail the form and your prescription to the address.
Based upon each patient’s prescription plan, additional questions may be required to complete the prior authorization process. Log in or register to access the forms. Find and print forms for mail order, claims, and medical questionnaire for tricare pharmacy benefits. Express scripts is administering this program on behalf of your medicare part d plan. 34202 please complete all information. You can ask your doctor to submit this form to us, or you can print and complete the form, then mail the form and your prescription to the address. New prescription your patient would like to receive their prescription medication by mail. If your address is different than what is on the form,.
New prescription your patient would like to receive their prescription medication by mail. Log in or register to access the forms. You can ask your doctor to submit this form to us, or you can print and complete the form, then mail the form and your prescription to the address. Find and print forms for mail order, claims, and medical questionnaire for tricare pharmacy benefits. Express scripts is administering this program on behalf of your medicare part d plan. If your address is different than what is on the form,. Based upon each patient’s prescription plan, additional questions may be required to complete the prior authorization process. 34202 please complete all information.
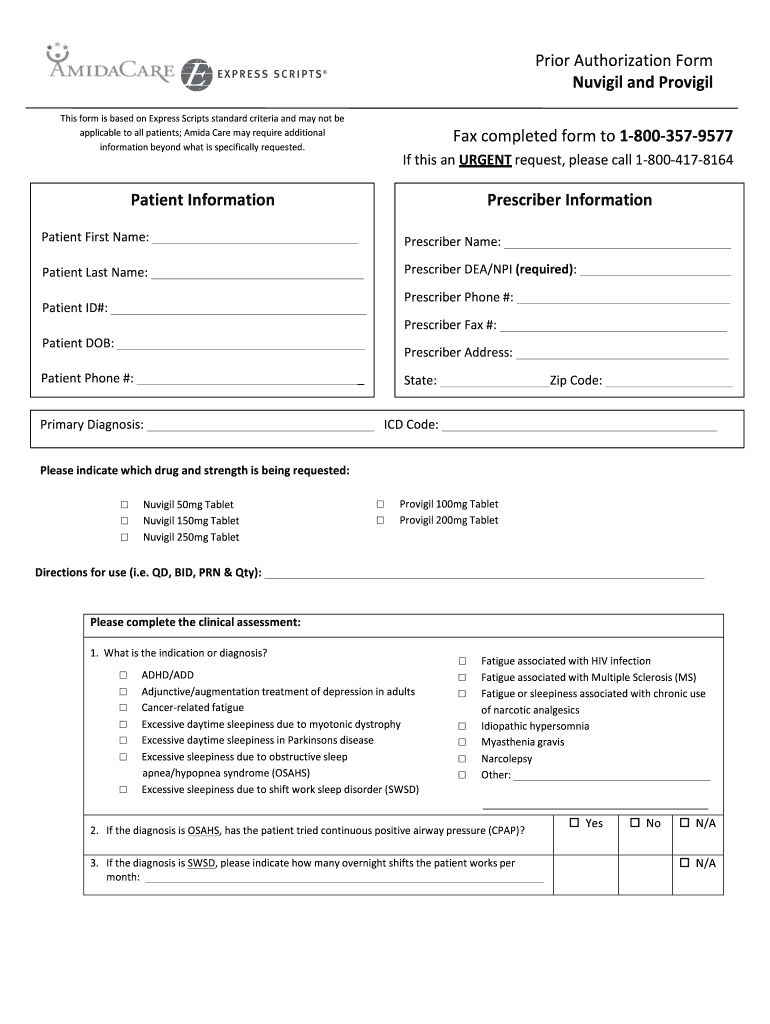
Express Scripts Prior Authorization Form for Fill Out and Sign
You can ask your doctor to submit this form to us, or you can print and complete the form, then mail the form and your prescription to the address. Find and print forms for mail order, claims, and medical questionnaire for tricare pharmacy benefits. Log in or register to access the forms. Express scripts is administering this program on behalf.
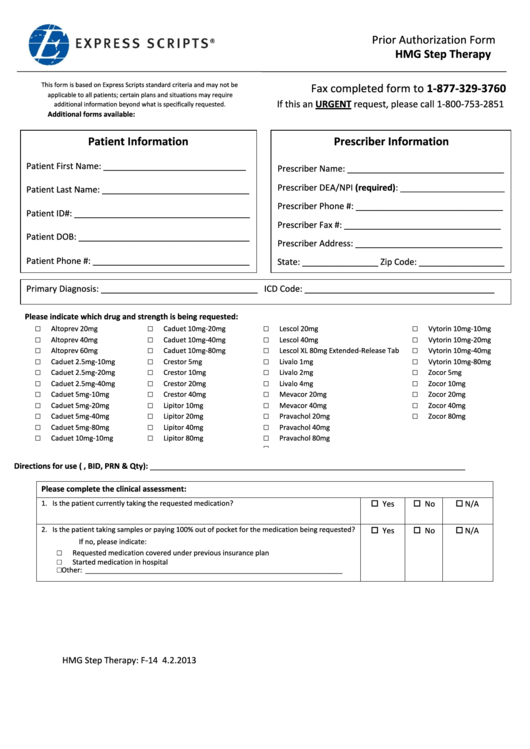
Express Scripts Prior Authorization Form Hmg Step Therapy printable
34202 please complete all information. You can ask your doctor to submit this form to us, or you can print and complete the form, then mail the form and your prescription to the address. Log in or register to access the forms. Express scripts is administering this program on behalf of your medicare part d plan. Find and print forms.
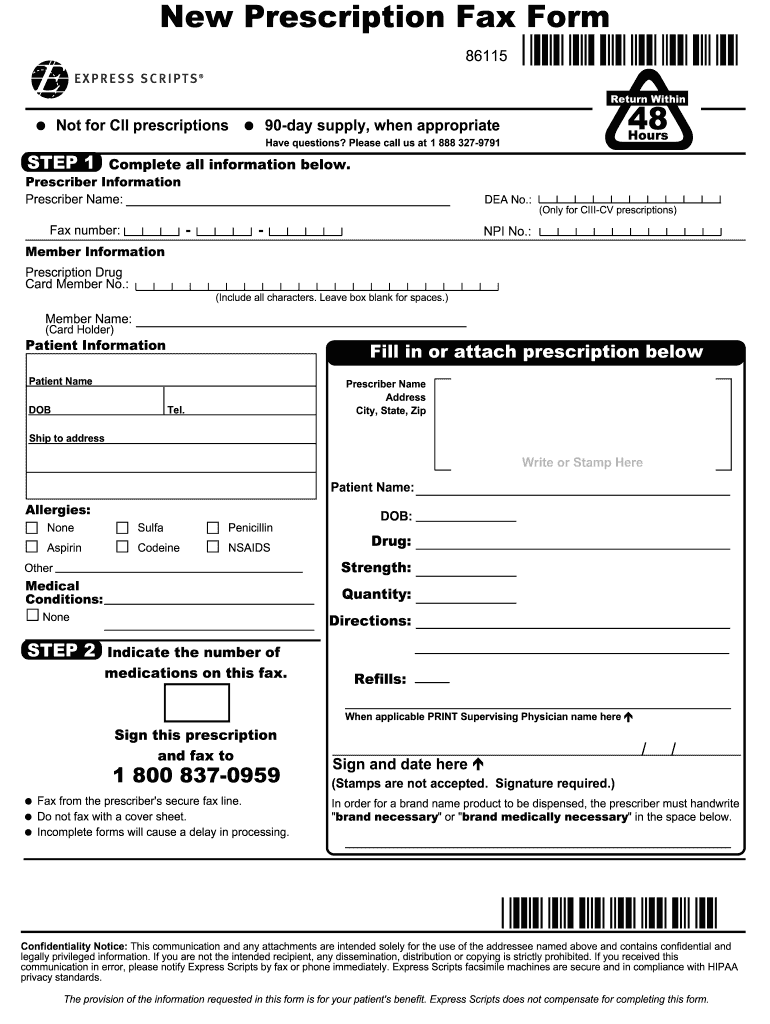
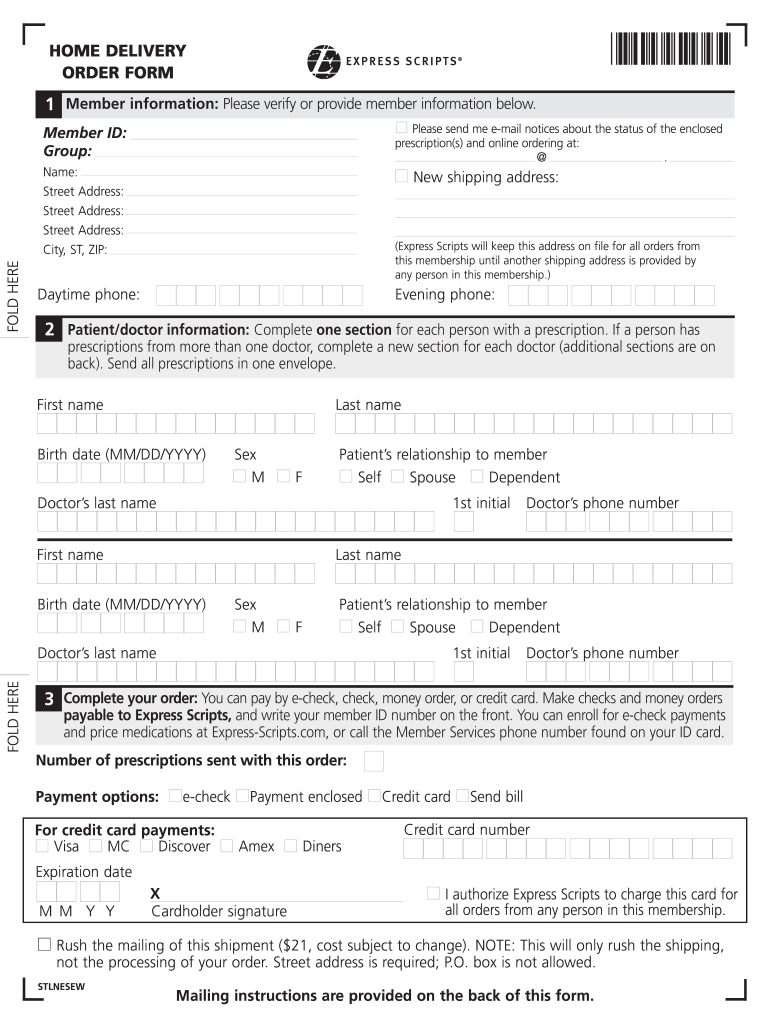
Express Scripts New Prescription Fax Form Fill and Sign Printable
Express scripts is administering this program on behalf of your medicare part d plan. New prescription your patient would like to receive their prescription medication by mail. Based upon each patient’s prescription plan, additional questions may be required to complete the prior authorization process. 34202 please complete all information. You can ask your doctor to submit this form to us,.
Express Scripts Prior Authorization Form 2023 Pdf Printable Forms
Find and print forms for mail order, claims, and medical questionnaire for tricare pharmacy benefits. Based upon each patient’s prescription plan, additional questions may be required to complete the prior authorization process. 34202 please complete all information. Log in or register to access the forms. New prescription your patient would like to receive their prescription medication by mail.
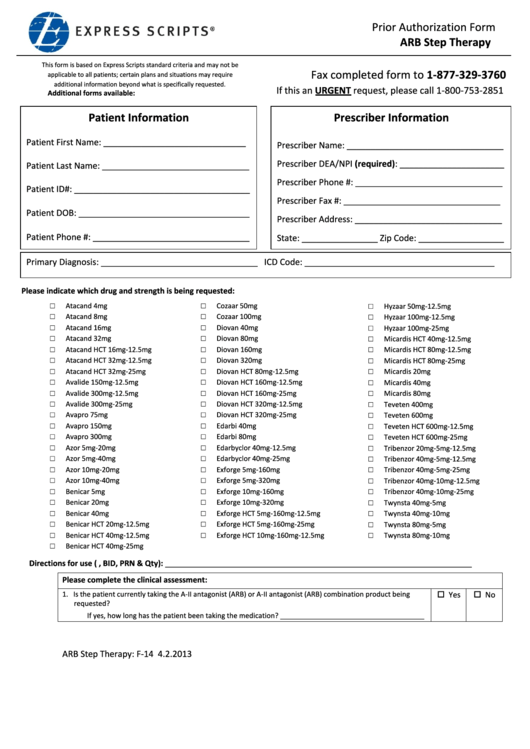
Express Scripts Prior Authorization Form Arb Step Therapy printable
New prescription your patient would like to receive their prescription medication by mail. Find and print forms for mail order, claims, and medical questionnaire for tricare pharmacy benefits. Log in or register to access the forms. 34202 please complete all information. Express scripts is administering this program on behalf of your medicare part d plan.

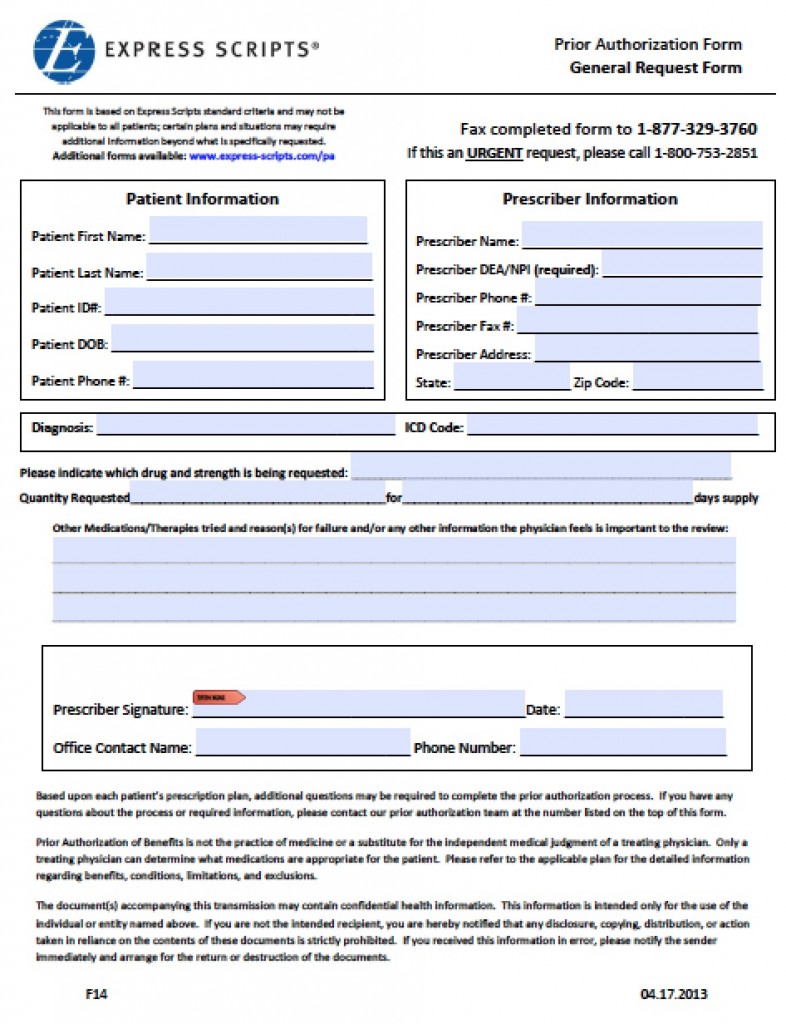
Fillable Online Free Express Scripts Prior (Rx) Authorization Form
Express scripts is administering this program on behalf of your medicare part d plan. New prescription your patient would like to receive their prescription medication by mail. 34202 please complete all information. You can ask your doctor to submit this form to us, or you can print and complete the form, then mail the form and your prescription to the.
Express Scripts Phone Number Template and guide airSlate SignNow
Express scripts is administering this program on behalf of your medicare part d plan. If your address is different than what is on the form,. 34202 please complete all information. Based upon each patient’s prescription plan, additional questions may be required to complete the prior authorization process. New prescription your patient would like to receive their prescription medication by mail.

Free Express Scripts Prior (Rx) Authorization Form PDF eForms
New prescription your patient would like to receive their prescription medication by mail. 34202 please complete all information. Log in or register to access the forms. If your address is different than what is on the form,. Express scripts is administering this program on behalf of your medicare part d plan.

Blank Express Scripts Form Fill Out and Print PDFs
If your address is different than what is on the form,. Based upon each patient’s prescription plan, additional questions may be required to complete the prior authorization process. New prescription your patient would like to receive their prescription medication by mail. 34202 please complete all information. Express scripts is administering this program on behalf of your medicare part d plan.
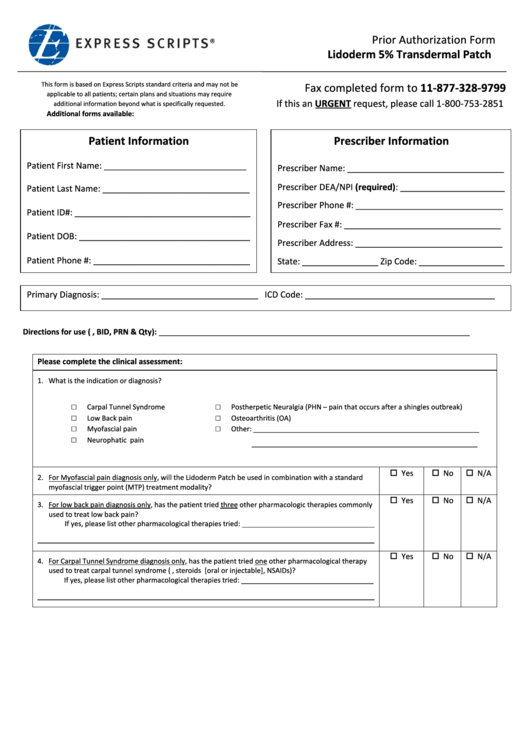
Express Scripts Prior Authorization Form Lidoderm 5 Transdermal
Based upon each patient’s prescription plan, additional questions may be required to complete the prior authorization process. Express scripts is administering this program on behalf of your medicare part d plan. Find and print forms for mail order, claims, and medical questionnaire for tricare pharmacy benefits. 34202 please complete all information. You can ask your doctor to submit this form.
34202 Please Complete All Information.
Log in or register to access the forms. Express scripts is administering this program on behalf of your medicare part d plan. Find and print forms for mail order, claims, and medical questionnaire for tricare pharmacy benefits. Based upon each patient’s prescription plan, additional questions may be required to complete the prior authorization process.
New Prescription Your Patient Would Like To Receive Their Prescription Medication By Mail.
If your address is different than what is on the form,. You can ask your doctor to submit this form to us, or you can print and complete the form, then mail the form and your prescription to the address.